SUBA-itraconazole (brandname TOLSURA) from Mayne-Pharma has recently become available and has some potentially useful absorption characteristics. This may be useful for some patients as absorption can be a major area of difficulty for itraconazole – it can be difficult to absorb. We wrote about this in 2017.
For deep mycoses, an initial itraconazole oral dose of 200 mg three times daily is recommended for the first 3 days to quickly achieve high serum and tissue levels. SUBA-itraconazole doses are only 100mg twice daily. Oral absorption of the capsule is significantly enhanced by food, whereas absorption of the oral solution is best on an empty stomach, neither affects the absorption of the SUBA-itraconazole. Absorption of the capsule is markedly depressed in those with mucositis, and in patients with acquired immunodeficiency syndrome (AIDS) because of enteritis, but this problem can be alleviated by using the solution or SUBA-itraconazole. SUBA-itraconazole has many fewer side effects (notably less nausea and diarrhoea than the oral solution.
WHO accepts rapid tests for life threatening fungal diseases aspergillosis and Pneumocystis pneumonia as ‘Essential Diagnostics’
The World Health Organisation, today issued its 2020 Essential Diagnostics list and included both rapid tests for invasive and chronic aspergillosis and Pneumocystis pneumonia.
The last few years have seen major steps forward in diagnostic accuracy and simplicity of tests for life-threatening fungal disease. Globally, aspergillosis affects over 10 million people while Pneumocystis affects approximately 500,000 people per year. Tests are mandatory for optimized clinical care – these infections are clinically subtle. Untreated most are fatal.
On behalf of millions of people affected each year, the Global Action Fund for Fungal Infections (GAFFI) applied for these tests to be included as Essential, using the 2-step procedure adopted by WHO. They were considered by the Strategic Advisory Group of Experts, this year using remote communications. The 3rd annual Model List of Essential in vitro Diagnostics was issued January[1] 29th 2021.
GAFFI had prepared the ground for these applications with an international consensus working meeting in Kampala, in April 2018, and subsequently published a paper summarizing the meetings conclusions[2] .
In addition to critically important fungal disease diagnostics, the WHO SAGE IVD group have evaluated PCR and other molecular tests for Covid-19. Several different assays are included in the 3rd Essential Diagnostics’ list, with commentary on their clinical and public health application.
The tests endorsed as essential were:
1. Aspergillus antigen – critical for the diagnosis of invasive aspergillosis which affects leukaemia, lung cancer, intensive care patients (including those with influenza and COVID-19), HIV and those admitted to hospital with COPD. The test is most sensitive in bronchoscopy fluids from all patients and blood from leukaemia patients. It is far superior to culture.
2. Aspergillus antibody – critical for the diagnosis of chronic pulmonary aspergillosis which both mimics and complicates TB of the lungs. About 10% of TB patients have aspergillosis, not TB. Many patients with fungal asthma and Aspergillus sinusitis have positive Aspergillus antibodies too. Aspergillus antibody is 80-92% sensitive depending on the test used, again much more sensitive than culture.
3. Pneumocystis PCR – about 25% more sensitive than direct microscopy and 10% more sensitive than fluorescence microscopy, and the only test possible in young children with this infection. Pneumocystis jirovecii is a human only lung fungus that cannot be cultivated in the laboratory. PCR is a molecular test that has been sufficiently refined to be shipped to hot countries without dry ice, by some manufacturers. While doctors often suspect Pneumocystis pneumonia in AIDS, over-treatment leads to major drug side effects and no diagnosis and treatment is fatal.
It is unbelievable that as of today there are only three classes of antifungal drugs in clinical use for deep infections: azoles, polyenes (amphotericin-B) and echinocandins (four, if we count flucytosine). These drugs have been paramount in the fight against fungal infections and have saved many, many lives. However, their use is becoming restricted due to the surge in resistant isolates. Therefore, it is clear that new antifungal drugs are urgently needed. There is hope, nevertheless, as various antifungal drugs are currently being evaluated in clinical trials. The scientific, physician and patient communities are excited about the revolution that these new treatments will have on the management of infections. We believe that this should become a trend and novel drugs, particularly with novel mechanisms of action, should be constantly under development.
In the Manchester Fungal Infection Group we have recently characterised a promising new target candidate for drug development: methionine synthase. This protein is known to be essential for various fungal pathogens (including Aspergillus fumigatus, Candida albicans and Cryptococcus neoformans), which means that these fungi cannot live without it… at least in our petri dishes in the laboratory. However, if we aim to develop a new drug to target it, we need to be sure that inactivating methionine synthase will inhibit fungal growth inside a human body. In addition, it is important to understand the mechanism of action, as this may help to prepare for and mitigate the development of antifungal resistance against the new drug. These are the questions we have addressed in our recent study.
As it can be inferred from its name, methionine synthase forms methionine, one of the proteinogenic amino acids. It was expected that if we supplemented methionine to the fungi, we could be able to inactivate methionine synthase and they should be able to grow. But that was not the case, and is the reason why we call this protein “essential”. The question was, why is it essential? In our recent study we have taken quite a few different approaches to finally disclose that, when methionine synthase activity is blocked, there is a metabolic imbalance that causes a reduction in cell energetics. So, basically, the fungal cells cannot produce the energy they need and just stop growing. This is useful information that will help to decide the best treatment courses and combinations to prevent the development of resistance.
In addition, we have optimised a genetic system to mimic drug treatment in a living model of infection. Using this model, we have been able to show that targeting methionine synthase in an established infection confers a beneficial effect on the outcome. Therefore, we could conclude that targeting methionine synthase is a suitable strategy to treat aspergillosis infection.
In conclusion, we have validated methionine synthase as a promising target for the development of new antifungals. We will work now towards that aim.
Scott J, Sueiro-Olivares M, Thornton BP, Owens RA, Muhamadali H, Fortune-Grant R, Thomson D, Thomas R, Hollywood K, Doyle S, Goodacre R, Tabernero L, Bignell E, Amich J. 2020. Targeting methionine synthase in a fungal pathogen causes a metabolic imbalance that impacts cell energetics, growth, and virulence. mBio 11:e01985-20. https://doi.org/10.1128/mBio.01985-20.
The National Aspergillosis Centre is at the forefront of understanding the best ways to treat chronic forms of aspergillosis. Two papers published this month add to the body of knowledge about how newer azoles (posaconazole and isavuconazole) can be used in this patient group.
Attainment of therapeutic posaconazole serum levels during coadministration with rifampicin (Power et al, 2020)
Treating patients affected by co-infections of Aspergillus and Mycobacterium is notoriously difficult because of drug interactions: rifamycin antibiotics are known to switch on liver enzymes that lower the amount of itraconazole/voriconazole in the blood. Staff at the Infectious Diseases department of Wythenshawe Hospital (part of MFT) have expertise in treating both conditions and recently published 2 cases of patients with both NTM-PD and CPA, who were treated twice daily with 300 mg delayed-release posaconazole. Both patients tolerated and responded well to the treatment.
Isavuconazole is the newest azole antifungal and was approved for invasive aspergillosis, but less is known about possible side effects among CPA patients, who tend to be immunocompetent and receive treatment for many months. Usually 200 mg daily is prescribed, but here they found that a lower dose (100 mg) was less likely to give side effects and gave a satisfactory level of the drug in the blood. Another study by Furfaro et al (2019) found that around 1 in 3 patients on 200 mg daily isavuconazole experienced side effects (mainly gastrointestinal).
Here’s our choice of review article highlights this month.
Diagnosis of severe respiratory infections in immunocompromised patients. Azoulay et al., 2020.
This review focuses on the diagnosis of severe respiratory infections in immunocompromised patients. Special attention is given to newly validated diagnostic tests designed to be used on non-invasive samples or bronchoalveolar lavage fluid and capable of increasing the likelihood of an early etiological diagnosis.
This article gives an overview of the mechanisms of action of currently used antifungals, as well as their spectrum of activity, clinically relevant pharmacological features, drug-drug interactions, and frequent side effects, all of which should inform the choice of agent when managing invasive fungal infections.
This paper reviews recent data on the composition and synthesis, influence of the components of the cell wall in fungi-host interaction and the role as a target for the next generation of antifungal drugs in yeasts and filamentous fungi (Aspergillus).
Each month we choose a handful of papers that stood out to us as highlights. Let us know if you think a particular piece of research should feature.
Levels of evidence supporting clinical practice guidelines on invasive aspergillosis. Tejada et al., 2020.
This paper is the first study analysing the quality of evidence supporting invasive aspergillosis guidelines. In evaluating the level of evidence (LOE) supporting recommendations in clinical practice guidelines (CPGs) of invasive aspergillosis (IA) it reports that among 238 strong recommendations, only 57 (24.0%) were supported by LOE A (multiple randomized controlled trial (RCT) or meta-analysis). When comparing recent CPGs with previous versions, the proportion of recommendations supported by LOE A did not significantly increase over time. The authors conclude that IA is a condition with an urgent unmet clinical need for more high-quality randomized trials.
Impact of high baseline Aspergillus-specific IgG levels on weight and quality-of-life outcomes of patients with chronic pulmonary aspergillosis. Bongomin et al., 2020.
This retrospective study evaluates the impact of quantitative baseline Aspergillus-specific immunoglobulin G (IgG) serum levels on weight changes of patients with chronic pulmonary aspergillosis (CPA) under antifungal treatment. A very high Aspergillus IgG may confer a higher likelihood of weight gain as a key, objective marker of clinical response, if patients can tolerate 12 months of antifungal therapy.
Clinical outcomes of patients with chronic pulmonary aspergillosis managed surgically. Setianingrum et al., 2020.
Surgical resection is one treatment modality for chronic pulmonary aspergillosis (CPA), and sometimes a preoperative presumption of lung cancer turns out to be CPA. This study audits surgical experience with regard to risk factors for relapse, and the value of postoperative monitoring of Aspergillus-immunogolubulin G (IgG) titres. It concludes that surgery in selected patients with CPA can have favourable outcomes. Relapse is common after surgical treatment of CPA but can be minimized with antifungal therapy, emphasizing the importance of an accurate diagnosis prior to surgery.
Club Cell TRPV4 Serves as a Damage Sensor Driving Lung Allergic Inflammation. Wiesner et al., 2020.
Wiesner et al. show a secreted fungal protease allergen of humans induces inflammation in mice with hallmarks of allergic asthma. The protease damages junctions of bronchiolar epithelial club cells, which the mechanosensor and gated calcium channel TRPV4 detects. Calcineurin mediates the calcium signaling and cellular alarms initiating lung allergic inflammation.
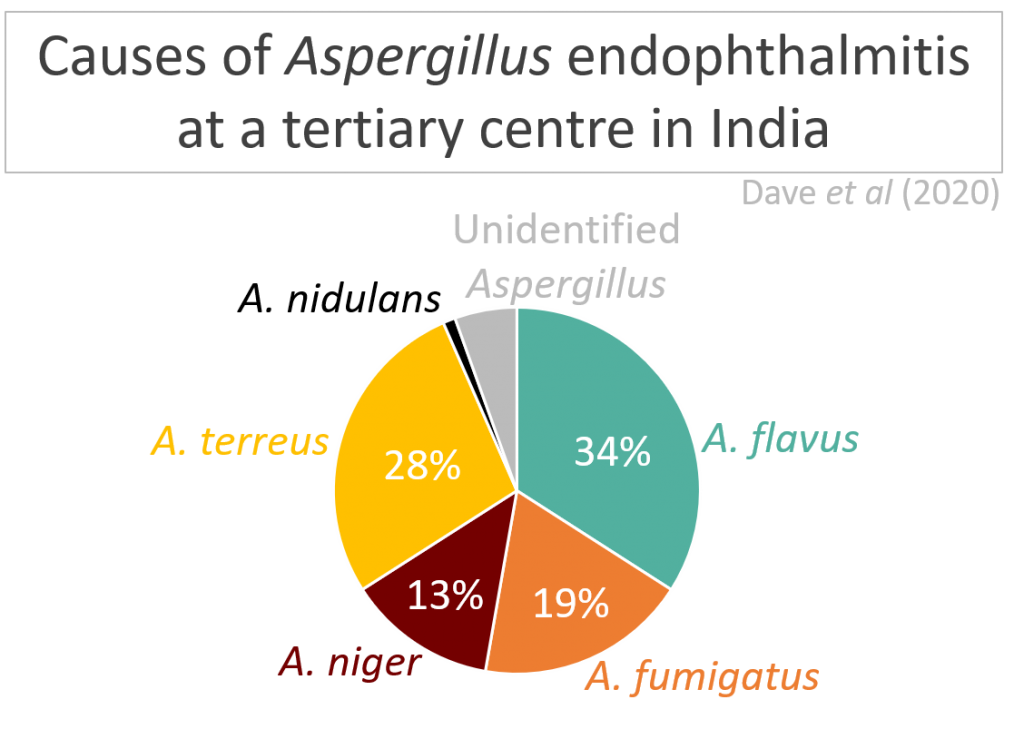
Aspergillus Endophthalmitis: Clinical Presentations and Factors Determining Outcomes. Dave et al., 2020.
This retrospective, interventional, multicentric case series describes the clinical presentations, management and factors determining outcomes of Aspergillus endophthalmitis, an eye infection. It reports trauma and intraocular surgery as common causes. The common infecting fungi are Fusarium and Aspergillus species for exogenous endophthalmitis, the latter having high ocular morbidity and poor outcome.
Veterinary research
Development of a comprehensive protein microarray for immunoglobulin E profiling in horses with severe asthma. White et al., 2019.
This study reports that protein microarrays can be used for large-scale IgE mapping of allergens associated with the environment of horses. This technology provides a sound platform for specific diagnosis, management, and treatment of severe equine asthma (SEA). SEA is a prevalent, performance-limiting disease associated with increased allergen-specific immunoglobulin E (IgE) against a range of environmental aeroallergens.
Here’s our choice of review article highlights this month.Treatment of allergic bronchopulmonary aspergillosis: from evidence to practice (Dhooria et al., 2020) This review illustrates the treatment pathway for ABPA in different situations, using a case-based approach. In each case, the options for treatment based on the available evidence from recent clinical trials is presented.
Detecting azole-antifungal resistance in Aspergillus fumigatus by pyrosequencing (van der Torre et al., 2020)Failure to detect azole-resistance dramatically increases the mortality rates of azole-treated patients. Despite drug susceptibility tests not being routinely performed currently, the authors of this review suggest including resistance testing whilst diagnosing Aspergillus disease. It also describes current diagnostic methods and highlights the potential of pyrosequencing to aid in a diagnosis complete with a resistance profile to improve clinical outcomes.
Role of lipid transporters in fungal physiology and pathogenicity (Rizzo et al., 2019)This review focuses on the structural and biological aspects of ATP-driven lipid transporters, comprising P-type ATPases and ATP-binding cassette transporters, (ii) the role of these transporters in fungal physiology and virulence, and (iii) the potential of lipid transporters as targets for the development of novel antifungals. These recent observations indicate that the lipid-trafficking machinery in fungi is a promising target for studies on physiology, pathogenesis and drug development.
Each moth we choose a handful of papers that stood out to us as highlights. Let us know if you think a particular piece of research should feature!.
Deep cutaneous fungal infections in solid-organ transplant recipients (Galezowski et al., 2020) This retrospective, observational, multicentre study was conducted in France to determine deep cutaneous fungal infections (DCFIs) diagnostic characteristics and outcomes with treatments in adult solid-organ transplant recipients. It describes the diversity and occurrence frequency of DCFIs. Phaeohyphomycoses were the most frequent DCFIs, representing a prevalence of 46%. Aspergillus species represented 8.7%.
Prevalence of fungal infection in nasal polyposis – A cross-sectional study, conducted at a tertiary care hospital in Karachi (Qaisar Sajjad et al., 2020) This cross sectional study, carried out from October 2010 to January 2015 on 221 patients in a tertiary care centre in Karachi was undertaken to determine the prevalence of fungal infections in nasal polyposis. Data was collected, a descriptive analysis was performed and a Computed Tomography (CT) grading was done. On the basis of histopathology, 90 (40.7%) patients were found to have fungal infection.
Functional characterization of clinical isolates of the opportunistic fungal pathogen Aspergillus nidulans (Bastos et al., 2020)Aspergillus nidulans has mainly been studied in the context of chronic granulomatous disease (CGD), with characterisation of clinical isolates obtained from non-CGD patients remaining elusive. This study reports a detailed biological characterisation of two A. nidulans clinical isolates (CIs), obtained from a patient with breast carcinoma and pneumonia and from a patient with cystic fibrosis that underwent lung transplantation, and compared them to the reference, nonclinical FGSC A4 strain. Differences in metabolic responses, growth rates and other strain-specific virulence traits and pathogenicity are described.
Diversity of secondary metabolism in Aspergillus nidulans clinical isolates (Drott et al., 2020) Despite its importance, there is little information about the natural diversity of secondary metabolism (SM) in A. nidulans. This paper describes six novel clusters that contribute to the considerable variation in both biosynthetic gene clusters content and SM production within A. nidulans. The authors emphasize that A. nidulans may also be a strong model to use within-species diversity to elucidate regulatory cross talk, fungal ecology, and drug discovery systems.
Exposure to mold proteases stimulates mucin production in airway epithelial cells through Ras/Raf1/ERK signal pathway. (Wu et al., 2020). This paper seeks to understand the underlying molecular mechanisms of airway obstruction and immune hyper-responsiveness caused by mucus overproduction in A.fumigatus induced lung diseases. It identifies and describes a novel downstream signal pathways that mediate A.fumigatus induced mucin production in airway epithelial cells. The discovery of this novel pathway contributes to the understanding of the pathogenesis of fungal sensitisation in allergic diseases such as fungal asthma.
Influenza can be complicated by invasive aspergillosis, as first described in 1952. About 35% of critically ill patients with COVID-19 are treated with corticosteroids and we know from meta-analyses that these patients have nearly double the mortality, lower ICU stay and more secondary infections, probably including aspergillosis (Rodrigo et al., 2015 and Ni et al., 2019). This link with corticosteroids is likely with COVID-19. Aspergillus antigen testing of respiratory fluids should be routine for these very ill patients.
Research into COVID-19 is taking place at an incredible pace but there is still much we don’t know. One key unknown is the frequency and impact of co-infections. Gangneuxet al. highlights the fact that invasive fungal infections are still rarely reported and may be underdiagnosed. It reports what is not known and what should be done.
Studies are starting to emerge reporting fungal co-infection rates. Koehler et al. published this week that clinicians caring for patients with ARDS due to COVID-19 should consider invasive pulmonary aspergillosis and subject respiratory samples to comprehensive analysis to detect co-infection. They noted that five of 19 critically ill patients (26%) developed COVID-19 associated invasive pulmonary aspergillosis. A pre-published report from Alanio et al. found putative IPA in almost one third of successive critically ill COVID-19 patients (not yet peer-reviewed). A further early release article describes a fatal case of invasive pulmonary aspergillosis in an immunocompetent patient in France who had severe coronavirus disease–associated pneumonia (Blaize et al., 2020).
As further research is undertaken we will collate it and make it available on the LIFE Worldwide website. The page will be updated as more information becomes available.
While less common than bacterial eye infections, fungal infections can lead to worse outcomes, especially if diagnosis and treatment are delayed.
Corneal ulcers (keratitis) are a significant public health problem in low-resource settings where many people work in industries (e.g. farming, forestry) with a high risk of traumatic onculation of fungi into the eye, and patients may present later in the course of infection due to poverty. Prajna et al (2017) shared their experiences of carrying out clinical research at Aravind Eye Hospital (India) with these challenges.
Many systemic formulations of antifungals have limited penetration into the eyes. Some antifungals can be administered intravitreally, but amphotericin B can cause retinal toxicity at higher doses (Payne et al, 2010). Voriconazole is less toxic but requires more frequent injection(every 24 hours) than amphotericin B (every 48 hours).
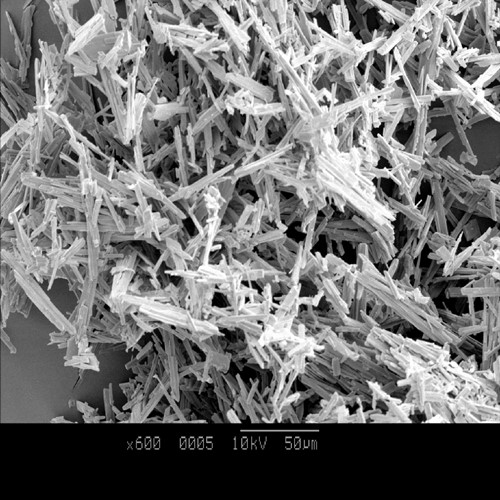
Fungal endophthalmitis is the infection of the interior parts of the eye (i.e. aqueous or vitreous humour), most commonly by Candida or Aspergillus. Two recent papers give insight into Aspergillus endophthalmitis.
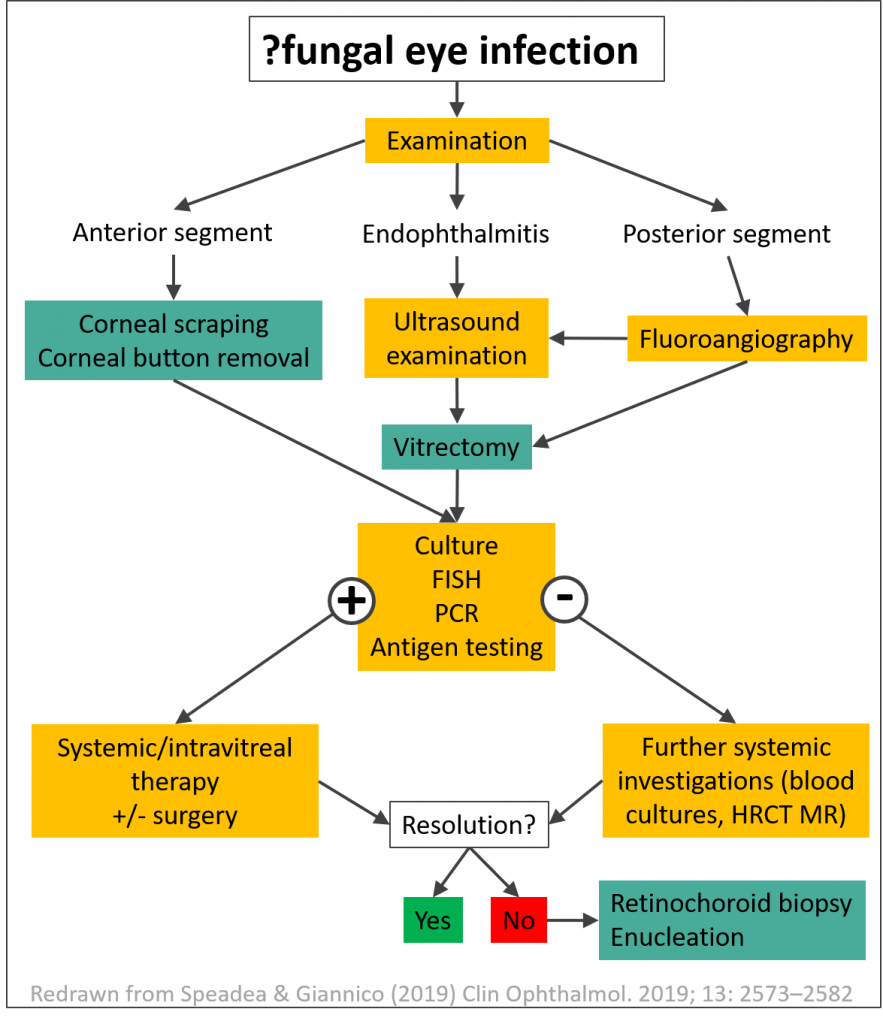
Dr Leopoldo Spadea and Dr Maria Giannico recently published a systematic review of the available diagnostic and management strategies for treating Aspergillus endophthalmitis. While there is a lack of serological tests, vitreous culture is often positive. Culture should be performed before starting antifungal treatment. Ultrasound examination is mandatory when the fundus cannot be explored by retinography.
Antifungals should be administered for at least a month, either systemically, intravitreally or in combination. Amphotericin B can cause retinal toxicity (especially at higher doses). Systemic voriconazole has relatively good penetration into the ocular compartment. Vitrectomy is often required, and enucleation may even be needed. Steroids should be used with caution as they can cause worsening of the infection.
Dr Vivek Dave and colleagues in India presented a large series of 91 immunocompetent patients with Aspergillus endophthalmitis. The most common causes were trauma (46%), surgery (42%) and endogenous (11%). 51 patients received amphotericin B only, 33 received voriconazole only, and 7 received both. They found that early vitrectomy was superior to vitreous tap alone, but outcomes were often poor. Corneal involvement and presence of fungal hyphae on microscopy were associated with worse outcomes.